- lauraclark849
- 2 days ago
- 15 min read
Updated: 8 hours ago
Peer Review Article | Open Access | Published 2 July 2026
Impact of Aseptic Dispensing on the Incidence of Nosocomial Infections: A Retrospective Study in a Hospital
Ajeng Prastyaning Apsari¹, Suci Hanifah² | EJPPS | 3102 (2026) | https://doi.org/10.37521/ejpps31201
Abstract
Contamination of sterile pharmaceutical products is a frequently overlooked source of nosocomial infections. This study aimed to evaluate the impact of implementing an aseptic dispensing program on the incidence of phlebitis in one local hospital. A retrospective ecological before–after study was conducted from January 2023 to November 2025. Aggregate data were obtained from the Infection Prevention and Control surveillance team and pharmacy documentation for hospitalized patients receiving intravenous therapy in the ICU and two regular wards. The pre-implementation period (January–December 2023, n = 4.400) was compared with the post-implementation period (July 2024–November 2025, n = 6,078). Data were analysed using the Chi-square test, relative risk (RR), and temporal trend analysis. The results demonstrated a reduction in phlebitis incidence from 0.250% to 0.099% (RR = 0.396; 95% CI: 0.151–1.038; p = 0.057), corresponding to a 60.4% relative risk reduction. Consistent decreases were observed in one ward (80.3%) and the ICU (100%) over 17 months of observation. An aseptic dispensing coverage of 54–60% was associated with optimal effectiveness. The aseptic dispensing program was associated with a substantial reduction in phlebitis incidence and may be considered an effective strategy for preventing nosocomial infections in Indonesian hospitals.
Keywords: aseptic dispensing; nosocomial infection; phlebitis; infection prevention; patient safety
Introduction
Healthcare-Associated Infections (HAIs) remain a major global public health problem. In developed countries, the prevalence of HAIs is approximately 7%, whereas in developing countries it reaches up to 15% ¹. In Indonesia, HAI prevalence has been reported as the highest in Southeast Asia, reaching 30.4%, with mortality rates ranging from 1.2% to 3.5% of all nosocomial infection cases ². The impact of HAIs extends beyond increased patient morbidity and mortality; they also prolong hospital length of stay by an average of 5–30 days and substantially increase healthcare costs ³,⁴.
One of the most frequently encountered forms of HAIs is phlebitis, an inflammation of the vein associated with intravenous catheterization ⁵. Its global prevalence varies widely, ranging from 2.3% to 67%, depending on the patient population and healthcare setting ⁶,⁷. Data from the Centres for Disease Control and Prevention (CDC) in 2017 indicated that phlebitis ranked as the most common nosocomial infection in Indonesia, with 16,435 cases among 588,328 at-risk hospitalized patients ⁸. If not managed appropriately, phlebitis can progress to serious complications, including thrombophlebitis, bloodstream infections, and sepsis ⁹.
The etiology of phlebitis is complex and multifactorial, involving mechanical factors such as catheter insertion trauma, chemical factors related to infusion solution pH and osmolarity, and biological factors associated with microbial contamination ⁹,¹⁰. Among these, microbiological contamination of sterile pharmaceutical preparations represents a frequently overlooked source of nosocomial infection, yet one that carries the potential to trigger outbreaks with severe or fatal consequences ²⁴,³². Epidemiological studies have estimated that 2–5% of HAIs are associated with contamination of sterile pharmaceutical products ⁶.
Aseptic dispensing refers to specialized techniques for compounding and preparing sterile medications designed to prevent microbial contamination. These practices are recommended by several international guidelines, including USP <797>, USP <800>, and the WHO Guidelines on Sterile Compounding ¹¹,¹². Such standards require dedicated facilities (e.g., laminar airflow workstations or biological safety cabinets), strict procedural protocols, and periodic validation to ensure product sterility ³,¹⁰. Microbiological studies have demonstrated contamination rates of 8–12% when intravenous preparations are compounded in non-aseptic environments, whereas the application of aseptic techniques can reduce contamination rates to below 0.1% ¹³.
In Indonesia, several studies have examined aseptic dispensing practices and phlebitis, albeit with differing focuses and limitations. Sari et al. evaluated the implementation of aseptic dispensing for non-cytostatic injectable drugs in Hospital X, West Java, and reported procedural compliance of only 44%, despite a relatively low contamination rate of 0.66% ¹⁴. Meanwhile, Mandias et al. (2023), using a case–control design, identified multiple risk factors associated with phlebitis among hospitalized patients ²¹. Although the theoretical relationship between aseptic dispensing practices and the prevention of nosocomial infections has been widely acknowledged ⁹,¹⁷, no study in Indonesia has quantitatively measured the direct impact of implementing an aseptic dispensing program on reducing nosocomial infection rates using a before–after design with an extended observation period.
This gap in the literature highlights an urgent need for research providing concrete evidence of the effectiveness of aseptic dispensing interventions within the context of nosocomial infection control in Indonesia. Therefore, this study aimed to: (1) evaluate differences in phlebitis incidence before and after the implementation of an aseptic dispensing program in a local hospital; (2) assess the consistency of the program’s effect over a prolonged observation period; and (3) identify the coverage/threshold of program which is effective. This study is expected to provide the empirical evidence in quantifying the impact of aseptic dispensing programs on reducing nosocomial infections and to serve as a reference for other hospitals considering similar interventions.
Methods
This study employed an ecological study design with a before–after (pre–post intervention) analytical approach based on aggregated data. The study was conducted at a hospital in Kutai, East Kalimantan, Indonesia. Data were collected retrospectively from the hospital information system, including nosocomial infection surveillance reports from the Infection Prevention and Control (IPC) team and dispensing records from the Pharmacy Department.
The study population comprised all hospitalized patients who received parenteral therapy. Inclusion criteria were inpatients receiving intravenous therapy in the ICU and two regular wards, namely Gaharu and Mahoni wards. The exclusion criterion was hospitalization during the transition period (January–June 2024), which was omitted to avoid data contamination during implementation. Total sampling was applied to all patients meeting the inclusion criteria during the pre-implementation period (January–December 2023) and the post-implementation period (July 2024–November 2025).
The analysed data consisted of aggregated monthly nosocomial infection incidence, including phlebitis, catheter-associated urinary tract infections (CAUTIs), and central line–associated bloodstream infections (CLABSIs). Data were collected at the ward level (ICU, Mahoni, and Gaharu) rather than at the individual patient level. These wards were selected due to their high volume of intravenous therapy and elevated risk profiles for nosocomial infections.
Total sampling was used throughout the study period. An a priori power analysis was not conducted because the study was retrospective and relied on existing data. With a total of 10,478 patients (4,400 in the pre-implementation period and 6,078 in the post-implementation period) and a baseline phlebitis prevalence of 0.25%, the study had limited statistical power to detect small differences but was considered sufficient to detect clinically meaningful reductions (≥50%). This limitation is acknowledged and considered in the interpretation of results.
The independent variable was the implementation of the aseptic dispensing program, while the dependent variable was the incidence of nosocomial infections. Study instruments included medical records, IPC surveillance data, and pharmacy dispensing documentation. Data were collected retrospectively from hospital information systems, medical records, and surveillance reports. The pre-implementation period was defined as the time before the establishment of a structured aseptic dispensing program, whereas the post-implementation period followed the introduction of standardized protocols, dedicated facilities, and trained personnel.
Data analysis included descriptive statistics to summarize sample characteristics, bivariate analysis to assess associations between independent and dependent variables, and correlation analysis to examine the relationship between aseptic dispensing coverage and nosocomial infection incidence.
Results
Table 1 presents the implementation timeline and key characteristics of the program throughout the study period. The pre-implementation period (January–December 2023) served as the baseline, during which no structured aseptic dispensing program was in place. The analysed post-implementation period comprised 17 months of observation (July 2024–November 2025), with a total of 23 months of documented dispensing data.
Table 1 Characteristic of Aseptic Dispensing Program
Phase | Period | Duration | Coverage* | Notes |
Pre- implementation | January-December 2023 | 12 months | 0% | Dispensing was implemented in the ward (no aseptic dispensing program) |
Transition | January-June 2024 | 6 months | 7,4%-32,7% (mean: 18%) | Pilot project and gradual implementation |
Post-implementation | July 2024 -November 2025 | 17 months | 54%-70,7% (mean: 59,5%) | Consistent program in three wards (ICU, Mahoni and Gaharu) |
*Coverage of prescription of sterile dosage forms which were implemented using aseptic dispensing
Based on Table 2, during the pre-implementation period (January–December 2023), a total of 11 cases of phlebitis were recorded among 4,400 patients with intravenous catheter placement (Table 2). However, there are no other types of nosocomial infections reported - either CAUTI or CLABSI.
Table 2 Comparison of nosocomial infection before and after implementation of aseptic
Parameter | Before (Jan-Des 2023) | After (Jul 2024-Nov 2025) | Differences |
Phlebitis incidence rate Number of Patients with IV Catheter Number of Phlebitis Cases Incidence Rate per 1,000 Patient | 4.400 11 (0,25%) 2,50‰ | 6,078 6 (0,099%) 0.99‰ | +1,678 -5 (-0,151%) -1.51‰ |
CAUTI incidence rate Number of Patient with Catheter Number of CAUTI Incidence rate (per 1000 catheter-days) | 3.105 0 0.00‰ | 2.944 0 0.00‰ | -161 0 0.00‰ |
CLABSI incidence rate Number of Central Line-days Number of CLABSI case Rate IADP (per 1000 CL-days) | 0 0 NA | 14 0 0.00‰ | -14 0 NA |
NA: not available data
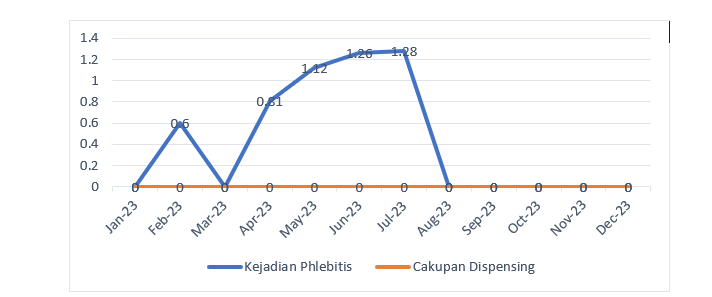
In contrast, phlebitis incidence exhibited considerable fluctuation, with the highest peak observed in July 2023 (1.28%) and several months recording zero cases. The mean monthly phlebitis incidence during the pre-implementation period was 0.42%, with substantial variability. Figures 1 and 2 illustrate the monthly time-series trend of phlebitis incidence from January 2023 to November 2025.

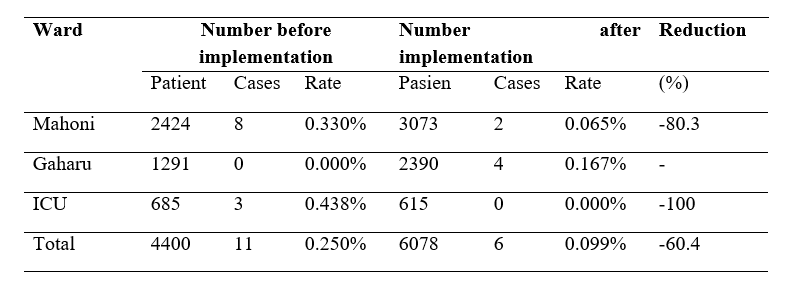
The distribution of phlebitis cases across hospital wards showed varying patterns, as summarized in Table 3. The Mahoni ward, which had the highest patient volume, experienced a reduction in phlebitis rate from 0.330% (8 cases among 2,424 patients) during the pre-implementation period to 0.065% (2 cases among 3,073 patients) during the post-implementation period, corresponding to an 80.3% reduction. The ICU demonstrated an even more pronounced effect, with phlebitis incidence decreasing from 0.438% (3 cases among 685 patients) before implementation to 0% (no cases among 615 patients) after implementation, representing a 100% reduction.
Table 3. Distribution of phlebitis in each ward
The comparison of phlebitis incidence proportions between the pre-implementation and post-implementation periods was performed using the Chi-square test. A 2×2 contingency table was constructed and is presented in Table 4.
Table 4. Table of contingency on phlebitis rate
Period | Phlebitis (+) | Phlebitis (-) | Total | Rate (%) |
Pre-implementation | 11 | 4389 | 4400 | 0.250 |
Post-implementation | 6 | 6072 | 6078 | 0.099 |
Total | 17 | 10461 | 10478 | 0.162 |
Chi-square Analysis
The Chi-square test revealed a χ² value of 3.606 (Yates’ continuity correction: χ² = 2.733) with 1 degree of freedom (df = 1) and a p-value of 0.057. Using a significance level of α = 0.05, this p-value indicates that the difference in the proportion of phlebitis between the pre-implementation and post-implementation periods was borderline statistically significant but did not reach the conventional threshold of p < 0.05. Therefore, the null hypothesis (H₀), which states that there is no difference in phlebitis incidence between the two periods, could not be rejected.
Effect Size Analysis
To quantify the magnitude of the association between the implementation of the aseptic dispensing program and the reduction in phlebitis incidence, several effect size measures were calculated, as presented in Table 5.
Table 5. Effect size of aseptic dispensing program toward the phlebitis rate
Effect size | Value | 95% Confidence Interval |
Relative Risk (RR) | 0,396 | 0,151 |
Risk Difference (RD) | 0,151% | - |
Number Needed to Treat (NNT) | 662 | 348-8,789 |
Cohen’s h | 0,037 | - |
Threshold of dispensing coverage
The Cohen’s h value for the difference in proportions was 0.037, which is classified as a small effect size according to conventional thresholds. However, within the context of patient safety and nosocomial infection prevention, a 60% reduction in relative risk remains clinically significant despite a small statistical effect size, especially for outcomes characterized as rare events.
Table 6. Comparison of phlebitis rate based on the coverage of dispensing
Threshold | Duration (months) | Total Patient in IV Catheter | Phlebitis Rate |
Coverage ≥60% | 10 | 3549 | 2 (0.056%) |
Coverage 54-59% | 7 | 2529 | 4 (0.158%) |
Total | 17 | 6078 | 6 (0.099%) |
Discussion
Implementation of Aseptic Dispensing Program
The aseptic dispensing service program was implemented gradually at this hospital beginning in January 2024. The program encompassed three main wards: the Intensive Care Unit (ICU), Gaharu and Mahoni (general medical ward). These wards were selected due to their high volume of intravenous therapy and patient populations with a high risk of nosocomial infections. Aseptic dispensing program has included reconstitution, dilution or IV admixture. It means all sterile drug preparation has been carried out in a sterile room and followed aseptic technique. A six-month transition phase (January–June 2024) was observed, during which dispensing coverage increased progressively from 7.35% to 32.66% of total inpatient prescriptions. The program reached a consistent implementation phase starting in July 2024, with stable coverage ranging from 54.27% to 70.66% (mean 59.5%), which was maintained through November 2025. The implementation of aseptic dispensing is closely aligned with pharmaceutical practice and the professional role of pharmacists in ensuring the sterility and quality of sterile medicinal product preparation ¹⁵. Aseptic principles in hospital setting extend beyond microbiological sterility to include control of chemical and particulate contamination, both of which may contribute to vascular irritation and adverse clinical outcomes ¹⁶,¹⁷.
Coverage of Aseptic Dispensing Program and Nosocomial Infection
Following consistent implementation of the aseptic dispensing program (July 2024–November 2025), the number of phlebitis cases decreased to 6 among 6,078 patients with intravenous catheters, corresponding to an incidence rate of 0.099% or 0.99 per 1,000 patients. The absolute reduction of 0.151% (1.51 cases per 1,000 patients) represents a relative risk reduction of 60.4% during the post-implementation period. These findings are in line with prior studies demonstrating that aseptic dispensing plays a critical role in reducing the incidence of phlebitis and other healthcare-associated infections ¹⁸. In addition to aseptic processing itself, the occurrence of phlebitis is also influenced by healthcare workers’ knowledge, behaviour, and adherence to established protocol ¹⁹. Therefore, robust quality control and assurance systems are essential to ensure that aseptic preparation practices effectively contribute to the prevention of healthcare-associated infections ²⁰.
However, no cases of catheter-associated urinary tract infection (CAUTI) were recorded during either study period, with a total of 3,105 catheter-days in the pre-implementation period and 2,944 catheter-days in the post-implementation period (Table 2). The use of central venous catheters was minimal throughout the study. No central line utilization was documented during the pre-implementation period, whereas 14 central line-days were recorded during the post-implementation period, with no cases of central line–associated bloodstream infection (CLABSI). Due to the limited occurrence of CAUTI and CLABSI events, meaningful statistical analysis for these outcomes was not feasible.
The majority of months during the post-implementation period recorded 0% phlebitis incidence, with only a few months reporting isolated cases. The mean monthly phlebitis incidence in the post-implementation period was 0.17%, representing a 59.5% reduction compared with the pre-implementation period. Following the consistent implementation of the aseptic dispensing program, phlebitis incidence demonstrated a more stable pattern and remained consistently lower over time.
The dispensing coverage within the range of 54–71% throughout the 17-month post-implementation period, indicating sustained and consistent program execution which has positive impact. The absolute reduction in phlebitis incidence of 0.151%, equivalent to 1.51 cases per 1,000 patients, reflects a clinically meaningful impact on nosocomial infection prevention. In hospitals with a high volume of intravenous therapy, such a reduction may translate into the prevention of a substantial number of phlebitis cases, some of which could otherwise progress to more serious complications ²¹. The Relative Risk (RR) of 0.396 indicates that the risk of phlebitis during the post-implementation period was 39.6% of that observed in the pre-implementation period, corresponding to a relative risk reduction of 60.4%. The Risk Difference (RD) of 1.51 per 1,000 patients reflects the magnitude of the absolute reduction in phlebitis incidence attributable to the intervention. The Number Needed to Treat (NNT) was 662, indicating that for every 662 patients receiving intravenous preparations compounded using aseptic dispensing, one case of phlebitis could be prevented. Although this NNT value appears relatively high, in the context of hospitals with a large volume of intravenous therapy, such a reduction represents a clinically meaningful impact, particularly given the potential progression of phlebitis to more serious complications. The number of those above effect size shows that implementation of aseptic dispensing is clinically meaningful.
However, this difference did not reach statistical significance, largely due to the small number of events (six cases in total). These findings support the interpretation that a minimum coverage threshold of approximately 54–60% already provides an optimal protective effect, and that increasing coverage to approximately 70% does not yield a substantial additional reduction in phlebitis incidence. The p-value close to the significance threshold suggests a potential error, likely attributable to the relatively small number of observed events (17 total cases of phlebitis). In patient safety research involving rare events, reliance solely on statistical significance may be misleading. In such contexts, effect size measures and clinical relevance are often more informative than p-values alone.
Variation in Outcomes Across Clinical Units
The heterogeneous reduction in phlebitis incidence across clinical units provides additional insight into factors that may moderate the effectiveness of the aseptic dispensing program. The Mahoni ward demonstrated an 80.3% reduction in phlebitis incidence (from 0.330% to 0.065%), while the Intensive Care Unit (ICU) achieved a 100% reduction (from 0.438% to 0%). These favourable outcomes are consistent with the expectation that aseptic dispensing confers a substantial protective effect, particularly in settings with high-risk patients and intensive intravenous therapy. In contrast, the Gaharu ward exhibited an apparent increase from 0% to 0.167%. As discussed previously, this finding most likely reflects surveillance bias or detection bias rather than a true increase in incidence. The absence of reported cases in the pre-implementation period (0 cases among 1,291 patients) may indicate under reporting rather than the absence of phlebitis. The implementation of the aseptic dispensing program was accompanied by continuous education of nursing and medical staff regarding the recognition and early reporting of phlebitis, which may have improved case detection, particularly for low-grade phlebitis that was previously overlooked.
This inter-unit variability underscores the importance of considering context-specific factors when interpreting the results. Differences in patient characteristics, types of intravenous medications administered, catheter care practices, and surveillance mechanisms may all influence observed incidence rates. The aggregate, unit-level analytical approach employed in this study does not fully control for these sources of variation, thereby contributing to residual statistical uncertainty.
Limitations
This study has several limitations that should be considered when interpreting the findings. Firstly, this study follows pre–post intervention design without a concurrent control group precludes definitive causal inference. The observed reduction in phlebitis incidence may have been influenced by other factors that changed contemporaneously with the implementation of the aseptic dispensing program. Although the sustained reduction over a 17-month observation period supports the interpretation that aseptic dispensing contributed to the decrease in phlebitis, residual confounding cannot be entirely excluded. Secondly, the relatively small number of phlebitis events (17 cases among 10,478 patients) resulted in limited statistical power to detect statistically significant differences. Consequently, the study may be subject to a Type II error, whereby a clinically meaningful effect did not reach conventional levels of statistical significance. Third, the analysis relied on aggregated monthly data at the ward level rather than individual patient-level data. This approach limited the ability to control for individual confounders (e.g., age, comorbidities, duration of intravenous therapy, catheter dwell time, and type of infused medications), to assess patient-level risk factors for phlebitis, and to explore potential interactions between aseptic dispensing and other determinants of infection risk. Lastly, differences in surveillance quality between the pre- and post-implementation periods may have introduced surveillance or detection bias. Underreporting of phlebitis events during the pre-implementation period cannot be ruled out, particularly given the enhanced staff education and heightened awareness of phlebitis following implementation of the aseptic dispensing program.
Conclusions
The implementation of an aseptic dispensing program was associated with a reduction in phlebitis incidence from 0.250% to 0.099% (RR 0.396; 95% CI 0.151–1.038; p = 0.057), which was sustained over 17 months of observation at a program coverage threshold of 54–60%. Although the difference did not reach conventional statistical significance (p > 0.05), the magnitude of effect indicates a 60.4% relative risk reduction, with consistent reductions across clinical units (Mahoni 80.3%, ICU 100%), suggesting a clinically meaningful benefit for nosocomial infection prevention.
Given the limited statistical power and the retrospective, pre–post study design, these findings should be interpreted with caution and cannot be considered statistically conclusive. Nevertheless, the observed effect size and temporal consistency support the potential role of aseptic dispensing as a patient safety intervention. Prospective, multicentre studies with individual-level data and appropriate control groups are warranted to confirm causality and to further delineate the impact of aseptic dispensing on healthcare-associated infections in hospital settings.
References
1. Organization WH. Global report on infection prevention and control: World Health Organization; 2022.
2. Goh LPW, Marbawi H, Goh SM, bin Abdul Asis AK, Gansau JA. The prevalence of hospital-acquired infections in Southeast Asia (1990-2022). The Journal of Infection in Developing Countries. 2023;17(02):139-46.
3. Allegranzi B, Nejad SB, Combescure C, Graafmans W, Attar H, Donaldson L, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. The Lancet. 2011;377(9761):228-41.
4. Haque M, Sartelli M, McKimm J, Bakar MA. Health care-associated infections–an overview. Infection and drug resistance. 2018:2321-33.
5. Annisa L, Hanifah S, Setiani P. Correlation Between the Use of Vesicant Medications and The Incidence of Phlebitis in Pediatric Ward. Journal of Pharmacy and Bioallied Sciences. 2024;16(Suppl 4):S4103-S6.
6. Braga LM, Parreira PM, Oliveira AdSS, Mónico LdSM, Arreguy-Sena C, Henriques MA. Phlebitis and infiltration: vascular trauma associated with the peripheral venous catheter. Revista latino-americana de enfermagem. 2018;26:e3002.
7. Marsh N, Webster J, Ullman AJ, Mihala G, Cooke M, Chopra V, et al. Peripheral intravenous catheter non‐infectious complications in adults: A systematic review and meta‐analysis. Journal of advanced nursing. 2020;76(12):3346-62.
8. Ekaputra OC, Fatmawati Y. Kepatuhan pelaksanaan standar operasional (SOP) pemasangan infus dengan kejadian phlebitis di Kudus. Indonesian Journal of Nursing Research (IJNR). 2022;5(1):9-20.
9. Gorski LA, Hadaway L, Hagle ME, Broadhurst D, Clare S, Kleidon T, et al. Infusion therapy standards of practice. Journal of infusion nursing. 2021;44(1S):S1-S224.
10. Oktavia Indrati RRPR, Suci Hanifah. Finding an accurate equation to estimate the osmolarity of parenteral nutrition for preterm baby. European Journal of Parenteral and Pharmaceutical Science. 2025;30(4).
11. Pharmacopeia US, editor General chapter< 797> pharmaceutical compounding—sterile preparations2023: The United States Pharmacopeial Convention Rockville, MD.
12. Organization WH. Guidelines on core components of infection prevention and control programmes at the national and acute health care facility level. 2020.
13. Austin PD, Elia M. A systematic review and meta-analysis of the risk of microbial contamination of aseptically prepared doses in different environments. Journal of Pharmacy & Pharmaceutical Sciences. 2009;12(2):233-42.
14. Sari N, Sumarny R, Laksmitawati DR, Nurcholis W. Implementation of Aseptic Dispensing for Non-Cytostatic Injectable Drugs in the Internal Medicine Inpatient Ward of'X'Hospital, West Java. Poltekita: Jurnal Ilmu Kesehatan. 2023;17(1):218-26.
15. Albesht H, Hanifah S, Bukhres S. Update on pharmacist role in sterile compounding in hospital. Jurnal Ilmiah Farmasi (Scientific Journal of Pharmacy). 2025;21(1):78-88.
16. Hanifah S, Ball PA, Kennedy RA. Nature of Precipitation Resulted from Intravenous Drugs Incompatibility. ASEAN Journal for Science and Engineering in Materials. 2025;4(2):151-8.
17. Achmad A. Uji Kesesuaian Aseptic Dipensing Berdasarkan Pedoman Dasar Dispensing Sediaan Steril Departemen Kesehatan di ICU dan NICU RSUD Dr. Saiful Anwar Malang. Pharmaceutical Journal of Indonesia. 2017;3(1):33-8.
18. Austin PDH, K.S; Elia, M; . Systematic Review and Metaanalyses of the risk of microbial contamination of parenteral doses prepared under aseptic techinques in clinical and pharmaceutical evnironment. Journal of Hospital Infection. 2015;91(4).
19. Ahmad IE, Rijal S, Haryati H. Analisis Faktor yang Mempengaruhi Kejadian Infeksi Nosokomial Flebitis di Rumah Sakit Umum Daerah Kabupaten Muna. Jurnal Surya Medika (JSM). 2020;5(2):42-53.
20. Beaney AM. Quality assurance of aseptic preparation services: Pharmaceutical Press; 2020.
21. Schreiber PW, Sax H, Wolfensberger A, Clack L, Kuster SP. The preventable proportion of healthcare-associated infections 2005–2016: systematic review and meta-analysis. Infection Control & Hospital Epidemiology. 2018;39(11):1277-95.
Authors
Ajeng Prastyaning Apsari¹, Suci Hanifah²
Master Degree of Pharmacy, Universitas Islam Indonesia
Department of Pharmacy, Universitas Islam Indonesia
Corresponding Author: Suci Hanifah
Email: suci.hanifah@uii.ac.id



Comments